.svg)
Health Notes
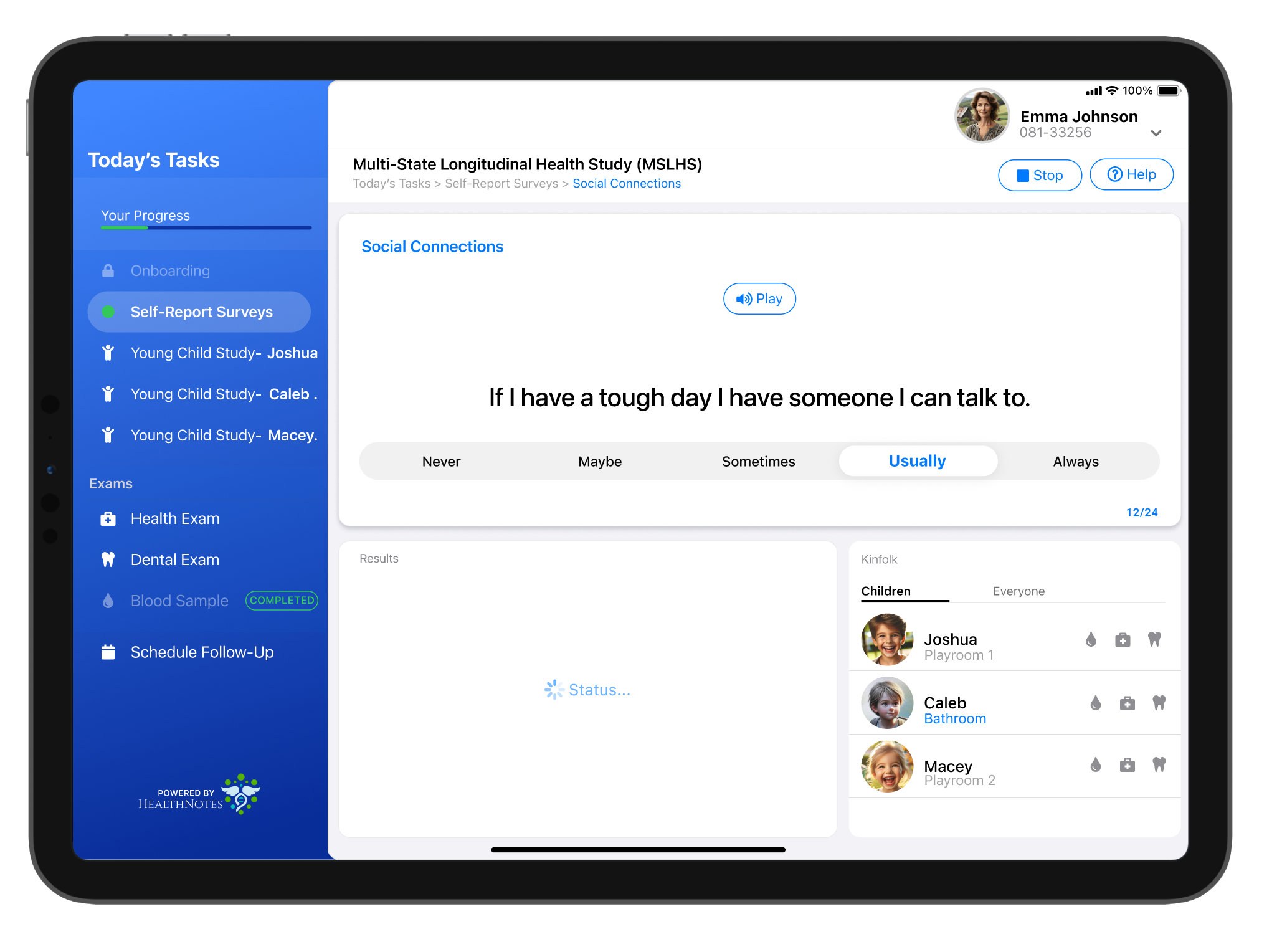
A speech-enabled tablet for rural clinics that turned dense health surveys into guided, spoken interactions, boosting completion to 96% and restoring trust in Appalachian communities.
Role
Design Lead
Design Lead
Timeline
8 weeks (field work + iterative design)
8 weeks (field work + iterative design)
Team
Researchers
(U. Pitt, WVU) Clinicians Developers Community liaisons
Researchers
(U. Pitt, WVU) Clinicians Developers Community liaisons
Compliance
HIPAA-compliant IRB approved
HIPAA-compliant IRB approved